Types of Top Surgery
Top Surgery, also referred to as gender-affirming upper surgery is an umbrella term for surgeries intended to help trans and gender diverse people align their physical characteristics with their gender expression and identity.
For the purpose of this blog post, we’re only going to cover chest construction procedures that reduce or remove chest tissue. In Canada, specifically in British Columbia, gender-affirming surgeries like top surgery are covered by the BC Medical Services Plan (MSP). In a previous post, I talked about the Surgery Readiness Assessment and steps you can take to pursue gender-affirming care.
The first three surgeries in this post are the most common ones, while the latter three will be less conventional options and techniques. I hope this helps you get a better idea of what might be the right option for you, but please continue to do more research as you work your way through this journey.
Double Incision Mastectomy
Often referred to as “DI” or “DI with nipple grafts” or “DI no nips” within the trans masc community, this is the most common type of top surgery because it’s a fairly reliable technique that can be used for a wide range of body shapes and sizes. Oftentimes, it’s the only option for people with larger bodies and/or larger chests.


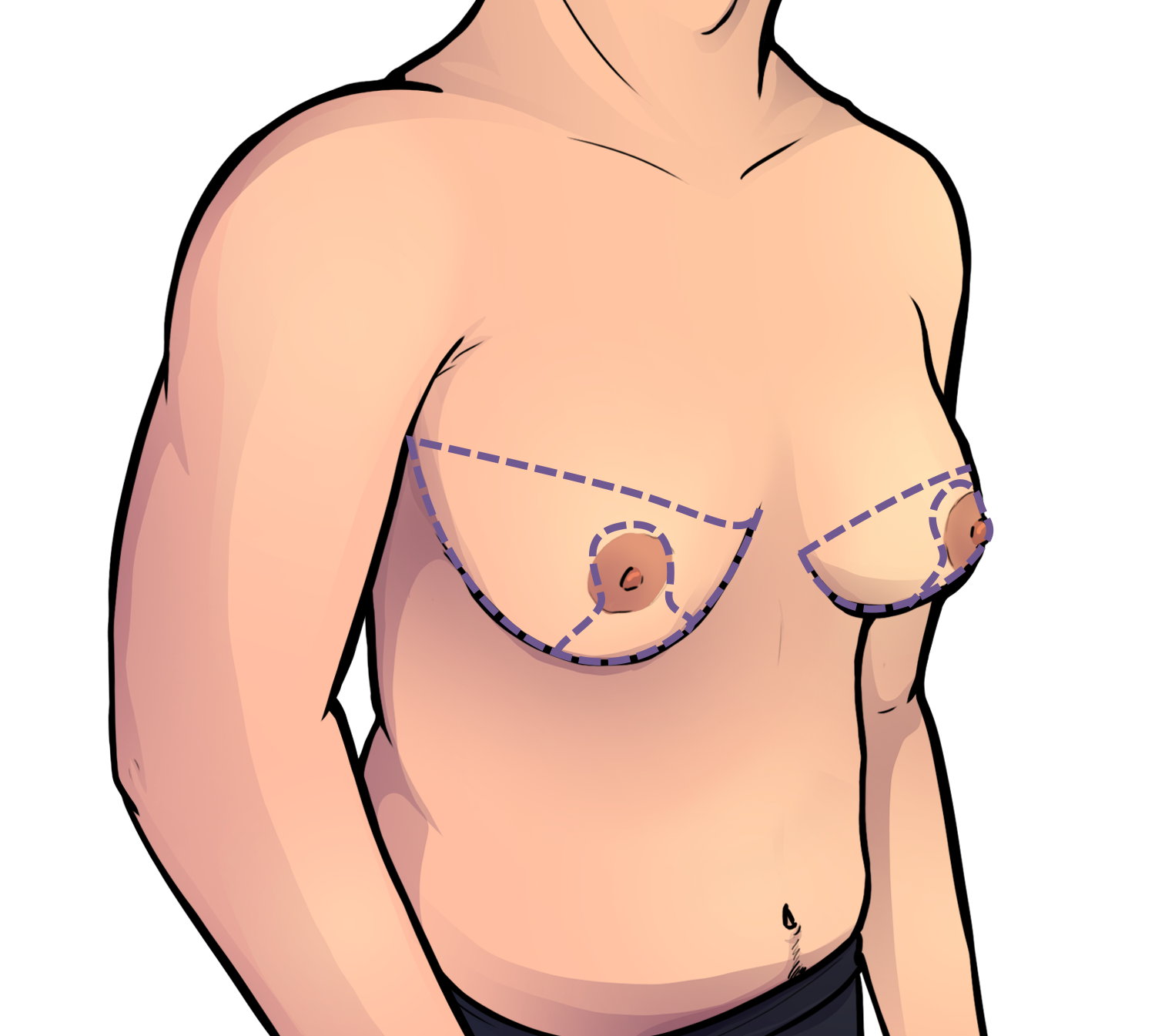
The procedure starts with an incision on each side of the chest, just below the pec muscles. For chests where the tissue is mounted very close to each other (as was the case for myself), the incision will cut all the way across the torso. From there, the surgery team will continue to cut around the breast tissue in order to remove the skin, fat, tissue and nipples.


Once all of the excess fat and tissue is removed, the skin on the upper and lower part of the chest is stitched together. This creates the hotizontal or U-shaped scars commonly associated with transmasculine individuals.


The level of straight versus curved scarring is influenced in part by patient preference, surgeon technique or expertise and patient anatomy. There is some wiggle room on how you can request your scars to look, but skin elasticity and body type will also play a part, so be sure to discuss your goals with your surgeon.
Within the realm of Double Incision Mastectomy, there are different options for how you might want to approach the appearance of your nipples (or lack thereof).
Nipple Grafts
A graft is basically a surgical implant of living tissue. Nipple grafts are created from the nipple and areola that had been removed during the mastectomy. They are typically resized to be smaller and have less of a protrusion before being stitched back onto the torso in a new position.
Surgeons use measurements to place the grafts, which they mark on your chest before the operation. By default, surgeons will tend to place the new nipples where they would typically be on a cis man’s chest. If you have specific preferences for where you would like your nipples to be placed, be sure to discuss that with your surgeon so that they can accommodate the specific size and placement you want.

“traditionally male” nipples sit really low and closer to the sides of the chest

“traditionally female” nipples are more centered
After the operation, the grafts are going to be extremely fragile in the weeks after surgery. There is a small chance of the grafts failing and post-op sensation is typically minimal.
Personally, it took me almost a year to feel like I genuinely had sensation in them, and it’s nowhere near what it was before top surgery. I had done a video testing out the sensation on my grafts, scars and chest, where the overall skin on my chest had full sensation while my scars had some sensation and my grafts had very little sensation.
Without Nipple Grafts
Another option is not to opt for nipple grafts at all. From there, some people can opt for restorative/cosmetic/3D tattoos after recovering from surgery, which creates the appearance of symmetrical, precisely placed nipples. Some people may also get artistic tattoos covering their chest while others will rock their chest as is.
A lot of it really depends on your preferences and what feels right for your gender identity
Keyhole
Another fairly common top surgery procedure is Keyhole, which results in very minimal scarring. Not everyone is eligible for it and it’s usually only done for people with a very small amount of chest tissue and good skin elasticity.
It starts with a small incision made just under or across the lower edge of the areola.


Fat and tissue is removed by liposuction through that incision. From there, skin will go inward to conform to the shape of the chest.


Because there is less control over nipple placement and size, adjustments can be considered as a second operation 3-12 months after the initial surgery. It also doesn’t address excess skin since the procedure mostly focuses on removing the underlying fat and tissue.
A major benefit to opting for keyhole is that it has such minimal scarring and it does have a higher chance of retained nipple sensation. If a person is eligible for keyhole and being “stealth” while shirtless in public is a priority, this would be a good procedure to opt for.
PERIAREOLAR
Often referred to as “peri” within the community, this procedure is essentially a middle ground between someone who isn’t quite eligible for keyhole, but still has good skin elasticity and moderate amounts of chest tissue.
It starts with incisions cut along the outer edges of the areola, followed by a second incision cut along a larger radius around the first incision.

This donut-shaped cut of skin is removed, followed by the underlying fat and tissue. From there, the nipple can be trimmed while still keeping the blood and nerve supply mostly intact.
Everything is stitched together, closing like a drawstring bag.


Similar to keyhole, peri results in much less visible scars than DI since the scarring will be just around the edges of the areola. There is a chance of skin puckering around the incisions, which can be fixed with a vertical incision just below the areola.
Because the nipple doesn’t get cut off completely, it also has a higher chance of preserved sensation than DI.
In British Columbia not all surgeons do this procedure, so be sure to ask and find out if it’s a procedure your surgeon is able and willing to do for you.
Three Less Common Top Surgery Procedures
The three surgeries we’ve covered so far are the most common ones, but there are also some less conventional approaches to top surgery, which I’m going to cover, but keep in mind that this isn’t an extensive list and there are other options still.
Inverted T-Anchor
The idea behind opting for the inverted T-anchor is to have a higher chance of preserved nipple sensation than DI, but it’s still not a guarantee that full sensation will come back. The technique is similar to what is commonly used in chest reductions, so this procedure is also sometimes referred to as a radical reduction.
Because the procedure doesn’t involve entirely removing the chest, you may not be able to achieve the same level of flatness as with DI, and there is less precision and control over nipple placement and size. The leftover tissue that might remain after this procedure may also affect the overall appearance of your chest if you intend to build up your pec muscles after surgery.

It starts with incisions on the lower part of the chest, just like with DI, but additionally, a thin flap of nipple and tissue is peeled back from the chest but not fully removed.
Once the excess fat and tissue is removed, the flap of nipple and tissue is put back against the chest, then the skin is stitched closed. This results in scars shaped like an inverted-T, hence the name of the procedure.


Fishmouth
This procedure results in scars higher on the chest, aligned with the areola and nipples. This has a “less natural” appearance compared to the previously mentioned procedures which for the most part aim to have scars blending into muscle lines or around areolas.
For someone whose priority is a chest that is neither stereotypically male or female, this could be a good option.


It starts with incisions around the areola and the chest tissue. Similar to inverted T-anchor and peri, it preserves the nipple while the fat and tissue under and around the nipples are removed. From there the upper and lower sections of skin are stitched together.


Because of how (at least for now) this procedure is less conventional, not all surgeons may be willing to do it and it may be necessary to explain what you want during a consultation and provide examples.
Chest Reduction
Another approach to top surgery that is typically more common in gender-nonconforming or nonbinary people is a chest reduction.
This would involve reducing the chest tissue, which would result in a smaller cup size, but not a completely flat chest. The technique used would tpiycally be similar to inverted-T anchor, but everyone has different bodies and different needs, so it would be important to discuss your goals and needs with the surgeon during your consultation.
Two main reasons for opting for a reduction instead of a full mastectomy would be that
a small chest but not a flat chest is what aligns most with your identity
if nursing in the future is a priority, the surgeon can prioritize preserving the nipples so that the ability to produce milk would potentially be preserved
In BC, chest reductions are covered by MSP through the Trans Care system. Coverage may be different in other provinces or countries.
Conclusion
Different people have different needs and there is a whole range of procedures and modifications to current procedures. Take the time to work through what you think feels the most right for you, and talk to different trans people who have experienced different surgeries and gotten different results.
Also keep in mind as you research your surgeon options that some of them specialize in only certain procedures while others are more open to customizing the procedure to better fit your goals. Different surgeons will also have different requirements. Some surgeons may have BMI limits and some may have specific restrictions and requirements around substance use.
A lot of research goes into this stage of a person’s gender-affirming journey, but I hope this helps. Feel free to also look through the links and resources I’m leaving below, most of which I used as references for this post.

References and Resources
http://www.phsa.ca/transcarebc/surgery/gen-affirming/upper-body-surgeries/chst-surg#Surgery
https://www.vancouvertopsurgery.com/double-incision-vs-keyhole
https://www.youtube.com/watch?v=Y20IcBCx8qQ
tw: graphic content, this is a video that shows the ACTUAL double incision mastectomy
https://www.youtube.com/watch?v=5tyZoqT-X5U
a 3D rendering of the Inverted T-anchor procedure
https://www.youtube.com/watch?v=vu_iYjdfXpg
a 3D rendering of the Fishmouth procedure